Globally, antibiotic resistance causes over 700,000 deaths annually. By 2050, it is projected to cause over 10,000,000 deaths annually. That is more than currently die from cancer each year. In 2019, the CDC and the Interagency Coordination Group on Antimicrobial Resistance released reports outlining the severity of antimicrobial resistance. The CDC report in particular outlined the top 18 pathogens most resistant to existing antibiotics and in need of urgent attention. One of the five listed at the highest level, “urgent threat”, is drug-resistant Neisseria Gonorrhoeae.
“The greatest possibility of evil in self-medication [with penicillin] is the use of too-small doses, so that, instead of clearing up the infection, the microbes are educated to resist penicillin and a host of penicillin-fast organisms is bred out which can be passed on to other individuals and perhaps from there to others until they reach someone who gets a septicemia or a pneumonia which penicillin cannot save.
In such a case the thoughtless person playing with penicillin treatment is morally responsible for the death of the man who finally succumbs to infection with the penicillin-resistant organism. I hope this evil can be averted.”
- Sir Alexander Fleming
Not all antimicrobial resistant infections will kill you. Some will just ruin the rest of your life.
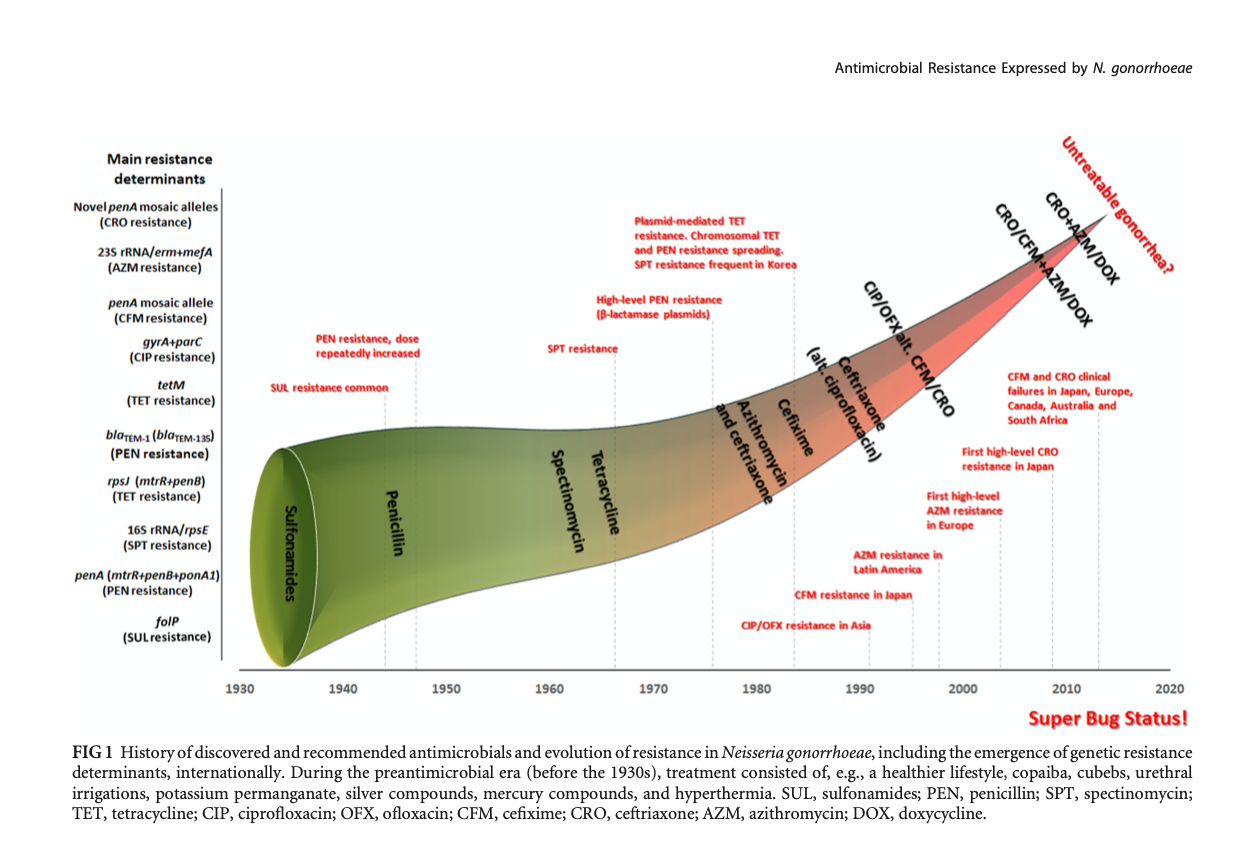
What was once an easily treated sexually transmitted infection now borders on being untreatable. A 2011 paper said, “During the last 70-80 years, N. gonorrhoeae had developed resistance to mainly all antimicrobials introduced for treatment of gonorrhea. Worryingly, the antibiotic treatment options now seem to be running out, and in the near future, gonorrhea may become untreatable in certain circumstances.”(1) That was 2011. Since then it has only gotten worse with the first documented case of "extensively drug resistant" NG diagnosed in 2014 and growing instances of treatment failure with extended spectrum cephalosporins. This means clinicians are left with combination treatments and the very real risk that gonorrhea will soon be untreatable. This is how critical AMR is to all of us.
AMR requires targeted treatments; and, the only method to determine an effective targeted treatment is AST, or antimicrobial susceptibility testing. However, not all tests are equal.
“Culture, the old “gold standard,” offers high sensitivity and up to 100% specificity (if appropriate species-verifying assays are applied) and is the only established method that enables complete AMR testing.”(2)
- Unemo & Shafer
Phenotypic testing is considered the gold-standard and it is what Acenxion is using. It is based upon analyzing the actual qualities or traits of the living organism itself. Even using our simple prototypes, when an antibiotic in our cassette kills the pathogenic microbe in that well, you know that combination of antibiotic and concentration is effective. This is the targeted treatment information clinicians and patients need with proof they can count on.
It is very fast, but that speed comes at a terrible price.
An alternative popular in research and development right now is genotypic (also called molecular) testing. It is very fast and frankly we don’t believe in it. The basic presupposition is that you can profile a pathogenic microbe by correlating genetic makeup alone to susceptibility while disregarding a cascade of processes that interplay at the biochemical and cellular level including:
“Most published evidence does not currently support use of WGS-inferred (whole genome sequence) susceptibility to guide clinical decision making (i.e. to replace routine phenotypic AST in most or all cases.)”(3)
- European Committee on Antimicrobial Susceptibility Testing
And then to double down this gamble, those genotypic tests rely on older data sets which generally only indicate the drugs that are least likely to help the patient. As Belkum, et. al. wrote in 2019, “Genotypic methods are surrogates for AST, and susceptibility has to be validated with phenotypic tests.”(4)
That paper was correct and we think of it in a much more straightforward way: A molecular test may be great at counting cards, but every player is unique and nature is constantly reshuffling the deck. This is why we’re committed to phenotypic testing. The very nature of gambling is that in the long run, the casino always wins. The proof that the same is true for antibiotic resistance is how quickly N. gonorrhoeae, M. tuberculosis, and a host of other pathogens are adapting to the antibiotics we have. The remaining effectiveness of antibiotics and the health of every patient is too important for gambling.
Sources
Acenxion Biosystems, Inc. All rights reserved. © 2025
Website design and development by Pixel Jam Digital
