It is probably fair to say that no one in the developed world can truly imagine life without antibiotics. They are ubiquitous in our lives and yet they are suffering as microbes develop more effective forms of resistance. Doctors provide us antibiotics as a companion to help fight an infection. Now, to slow down antimicrobial resistance, antibiotics need a companion too.

“Before the introduction of antibiotics, 40 percent of deaths in the UK were caused by infection: today, the figure is closer to 7 percent but is in danger of increasing if the efficacy of antibiotics is lost ."
- Figure given by Chief Medical Officer in presentation to The Parliamentary and Scientific Committee on 11 June 2013 at the House of Parliament, London, UK.
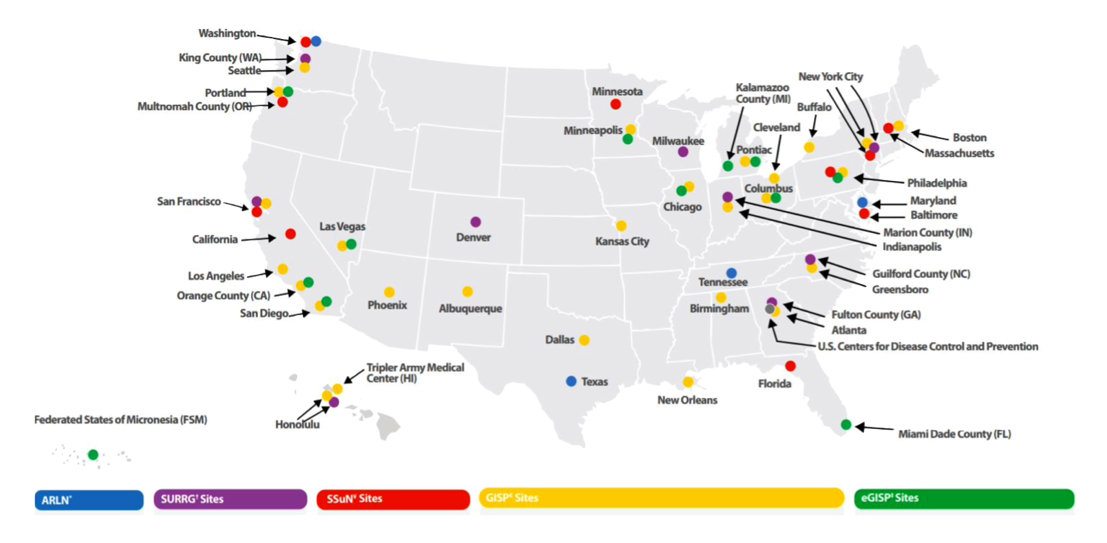
It starts with surveillance. In US there are over fifty locations tasked with AMR surveillance testing for gonorrhea. Different surveillance labs are also responsible for testing additional microbes. In every case these labs are the silent and often unknown heroes who help defend us and antibiotics from AMR. The unpleasant reality is that surveillance testing is a long, slow, and labor-intensive process. Because of this, some patients do not return for follow up testing or medical care. This is especially the case for at-risk populations and was the exact situation in Japan where a patient presented the first "extensively drug resistant" NG case showing resistance to ceftriaxone but didn’t return.
A key goal of ours is for Acenxion’s prototypes to be used in these labs – first through clinical trials as part of the proving grounds of our devices, then large trials using CLIA waivers, and eventually at full scale and volume allowing the surveillance network to enjoy a testing capacity and throughput rate previously unimaginable.
"Antibiotics are uniquely societal drugs because individual use [affects] others in the community and environment.”
- Dr. Stuart Levy, President of the Alliance for the Prudent Use of Antibiotics
Antibiotic stewardship is fundamentally taking the actions necessary to best optimize the use of antibiotics generally. This means prescribing antibiotics such that the infections are treated effectively, protecting patients from accidental harm caused by unnecessary or inappropriate antibiotic use, and minimizing antibiotic use to help combat antibiotic resistance.
We consider the use of broad-spectrum antibiotics necessary yet extremely suboptimal. Rather we believe that every use of an AST based targeted treatment is an act of antibiotic stewardship. Nowhere is this more apparent than in the treatment of sepsis. Please consider this passage from a paper by Charles Edmiston and his colleagues. This opinion has been verified by multiple infectious disease specialists. From the paper (emphasis added):
"The use of broad-spectrum, empiric therapy in treating BSIs (blood stream infections), including sepsis, has repeatedly been implicated as a contributor to antimicrobial resistance. Despite this, empiric therapy remains a mainstay of BSI—and particularly sepsis—treatment for several valid reasons. In fact, the international Surviving Sepsis Campaign Guidelines recommend “empiric broad-spectrum therapy with one or more antimicrobials for patients presenting with sepsis or septic shock to cover all likely pathogens (including bacterial and potentially fungal or viral coverage).”
This practice is based on the fact that, in many cases of primary BSIs [blood stream infections] the clinical picture belies a specific microbiologic diagnosis, leading healthcare providers to initiate therapy that covers a broad range of potential pathogens. Additionally, the acuity of BSIs and the knowledge that mortality directly correlates with time to effective therapy precludes waiting for ID and AST results. Thus, the longer the turnaround time (TAT) for those results, the longer it takes to de-escalate therapy and the more likely the empiric therapy is to contribute to downstream resistance. A vicious cycle ensues in which suspicion of resistant organisms as causative pathogens in BSI leads to the use of increasingly broad-spectrum antibiotics." (1)
Quickly switching from broad-spectrum antibiotics to a target treatment… results in faster and more effective elimination of infections. Acenxion’s prototypes are already demonstrating this is extremely achievable. Correct targeted treatments reduce AMR adaptation pressures on microbes and directly leads to extending the service life of our current antibiotic stock. And what this really means is more doses of effective antibiotics for more patients for many more years to come.
"The promise of precision medicine is that a deeper understanding of the mechanisms of disease can be a compass pointing toward better therapies.”
- Perez & Bonomo (2)
Precision is a hot topic in the medical research space. An earlier term was personalized. The notion is using additional information about the patient, their lifestyle, etc. to provide more effective health care. Currently, cancer is the area where precision medicine seems to be the most mature and a key element of precision treatments in cancer is the use of companion diagnostics. This is where a diagnostic tool aids a clinician in selecting the most ideal treatment for a patient. In the case of cancer there is a strong molecular component as it is the patient’s own body misbehaving in the case of cancer. Ultimately, we believe infections will be part of precision medicine as well.
“Precision” has an opportunity to play a strong role in dosage selection for at-risk populations – the elderly, those already sick, etc. At risk patient populations have highly variable pharmacokinetic and pharmacodynamic (PK/PD) responses, so having a rapid phenotypic AST test with a broad panel of concentrations for multiple antibiotics could show the clinician a larger number of effective targeted treatments and allow them to select the one which is not only highly effective for treating the infection, but is also most likely to reduce the risk of potential toxicity or complications from other prescription interactions.
“In general, most studies on pharmacokinetics (PK) have been performed in small groups constituted of persons who are normal in weight and height. Even in these studies, it is evident that there is a substantial interindividual variation in PK. In infected patients, the PK is further impacted by changed perfusion due to the inflammatory response. Previously, it has been an unspoken dogma that “one size fits all” when it comes to antibiotic dosing. However, studies have revealed that we are not achieving the serum concentrations expected by standard dosing.” (3)
Today, however, because phenotypic AST testing is too slow, there is no point in developing alternative concentration test panels for at-risk populations. All of this and so much more can change with the rapid, automated phenotypic AST system Acenxion is developing.
Sources
Acenxion Biosystems, Inc. All rights reserved. © 2024
Website design and development by Pixel Jam Digital
